
Cause of death: Vaccine-induced myocarditis?
I am concerningly seeing more and more patients with vaccine-related side effects at work. Presentations over the last month have included: a frozen shoulder (of the jabbed arm), systemic inflammation, blood clots, excessive facial sweating, total body fatigue and missed menstrual periods.
I have to note that all these patients were once previously ‘fit and healthy’ and though some suspected that the vaccines may have had something to do with their new ailment, the majority were either in denial or completely oblivious to any link between the two. Others have even asked me how they’d go about booking for a booster. Cognitive dissonance is still alive and kicking.
The Yellow Card scheme is run by the Medicines & Healthcare products Regulatory Agency and is the UK system for collecting and monitoring medication-related safety concerns. The scheme relies on voluntary reporting of suspected side effects to be reported by health professionals and the public. It is estimated that only 10% of serious reactions and between 2 and 4% of non-serious reactions are reported.
As of 20th of October 2021, for the UK, there have been 378,074 Yellow Cards reported for the Pfizer/BioNTech, AstraZeneca and Moderna vaccines combined. Taking that only 2-10% of reactions are only normally reported, this places the number of actual possible side-effects at around 3.5 million to 17 million cases in the UK.
COVID vaccine-related adverse events in the US is staggeringly high too, and it is pertinent to remember that these new vaccines haven’t even been in mass-circulation for more than a year. We have no idea what the long term implications of these vaccines are, we have no idea what further boosters will do.
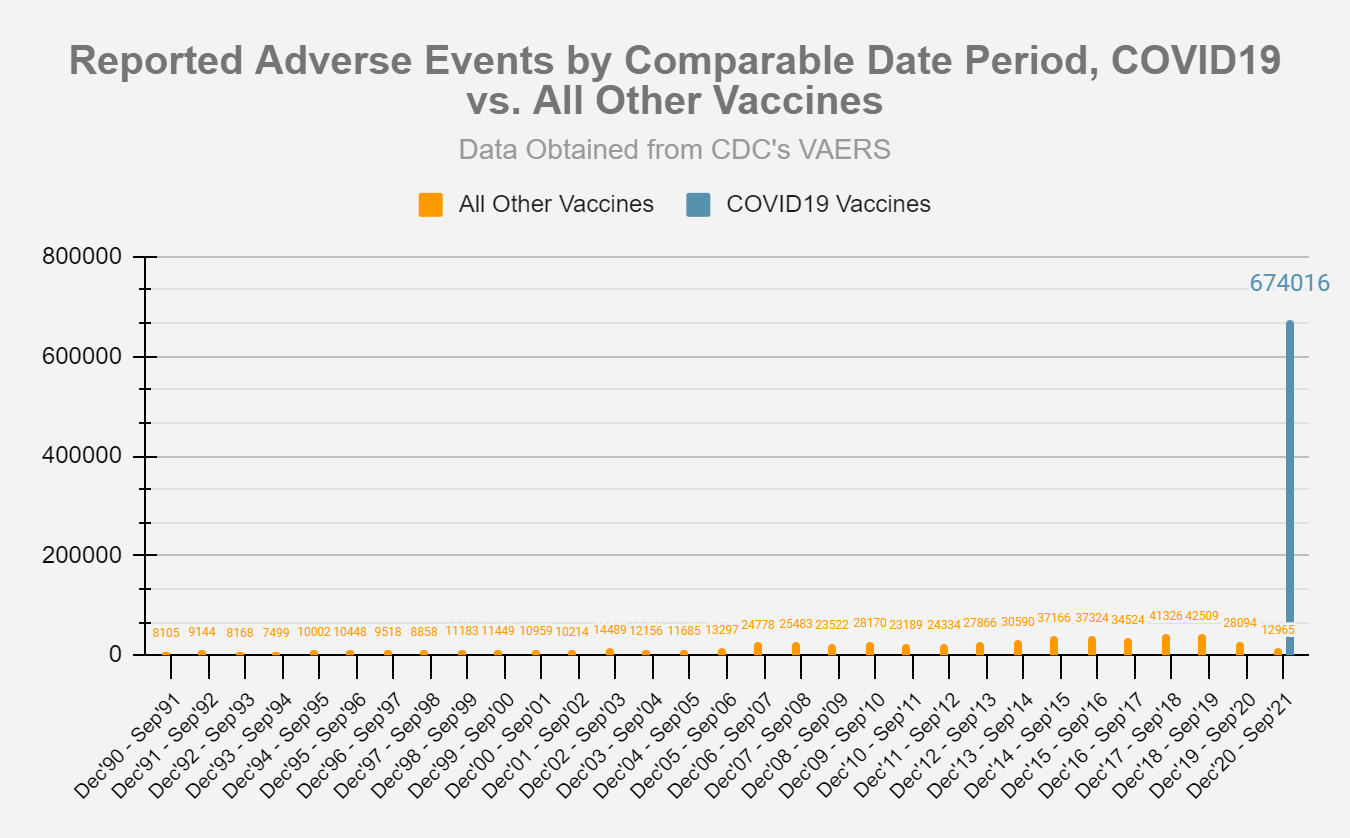
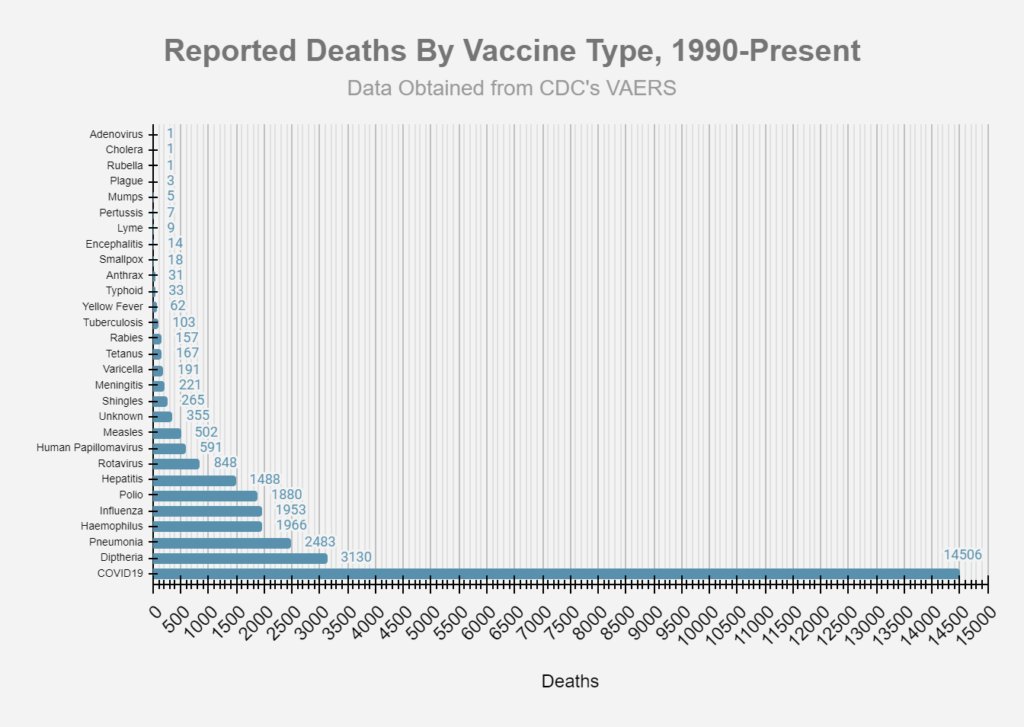
It’s not just side-effects, in the US, the total number of deaths associated with the COVID-19 vaccines is greater than the number of deaths associated with all other vaccines combined since the year 1990. What is going on?
How many more coincidental deaths before we wake up?
If you have been paying attention recently, you may have noticed an increasing number of news reports outlining the sudden tragic deaths of previously former healthy individuals. Some state that the individual had been fully vaccinated, whilst others do not delve into this detail. And mainstream media aren’t the only ones shying away from giving us the full picture.
It’s been hard to get clear-cut evidence of possible vaccine-related deaths. Secondary sources of information like the ones provided by the Centers for Disease Control and Prevention (CDC) and other government-funded agencies are littered with pro-vaccine biases, skewed information and straight-up lies.
In the UK, the definition of a “COVID death” is anyone who has died with a laboratory-confirmed positive COVID-19 test within (equal to or less than) 28 days of the first positive specimen date. Many have died with the virus, and not from it. The UK doesn’t have the data of those who have been harmed or suffered illness from a COVID-19 vaccination as this is not recorded on the death certificate.
With this information, I can only suspect that many thousands are inappropriately having the wrong cause of death written on death certificates. This is not only unscientific and deeply undignified, but it allows for others to suffer in the future. We must begin post-mortems.
At every level of the playing field, from pharmaceutical companies to the healthcare professionals administering the jabs, the data has been corrupted and fails to tell the vaccine recipient what really is going on. There is, and continues to be, blatant twisting of scientific data to fit a narrative, something known as propaganda. President Joe Biden, the ‘world’s most powerful man’, reportedly stated in July that “You’re not going to get COVID if you have these vaccinations.”. We are now waking up to this lie.
At the moment, to avoid biases, it may be best to rely on anecdotal evidence as well as raw figures. And both of these don’t look promising.
Look past COVID
Over the last two years, we have been conditioned to place COVID as the deadliest disease ever known to man. Constant reminders like daily death rates and masks were shoved in front of us month after month. There is no wonder why I see people now that are too worried to go into the hospital for cancer diagnosis and treatment.
This hyperacute focus on COVID meant other conditions were left on the wayside both in our minds and in reality. Cheap and effective medication and supplements that may have proven useful at prevention were vilified and banned. Gyms were closed and fast-food restaurants were left open. Was it ever about our health?
We are beginning to feel the repercussions of our mistakes now. The UK National Health Service is facing a health backlog like no other. Lockdowns increased the progression of chronic conditions and allowed poor mental health to fester. Delays in cancer screening back then meant more cancers and more pathologically progressed (and thus likely treatment-resistant) cancers now. Mass vaccinations have likely increased COVID cases. Many GPs at my practice have been off after contracting the virus again post-vaccination. That means more healthcare staff spending less time treating patients.
Future stricter healthcare vaccine mandates will be the last straw that breaks the camel’s back. And a collapsing healthcare service means longer waiting times, rushed medical care and unsafe procedures becoming the new normal for you and your family, if God forbid, you or they become seriously unwell.
We must remind ourselves that COVID isn’t the only disease to torment man. Whilst we were all glued to our screens distracted by COVID news and numbers, other worrying trends began to silently occur.
Young deaths
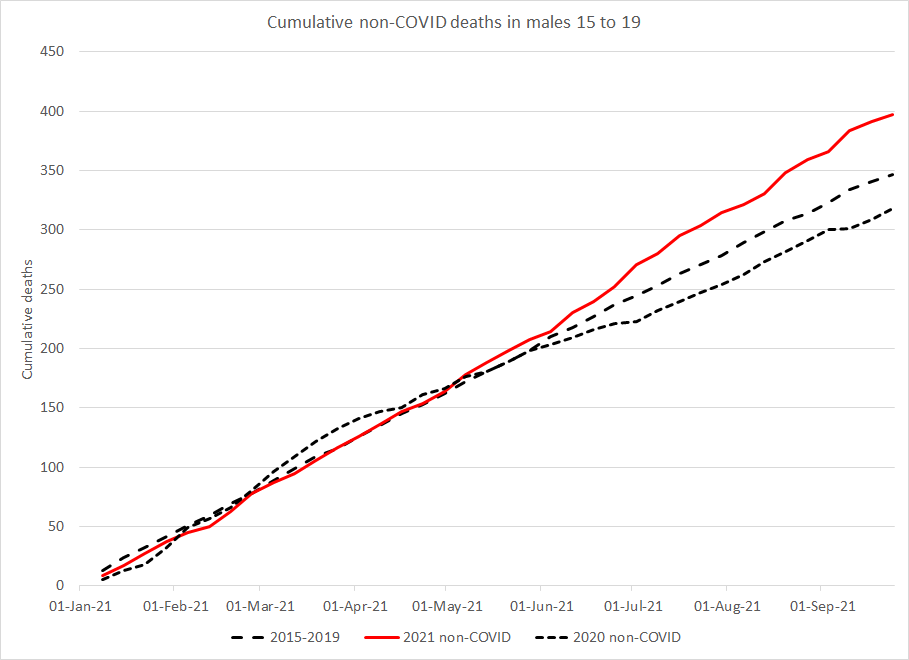
Mortality data from the Office for National Statistics (ONS) for England and Wales from the 1st of May 2021 until the 17th September 2021 shows a significant excess, particularly in the 15-19 year age group. This is between 16% or 47% above expected levels, depending on the baseline chosen. The data also shows that a disproportionate number of these excess deaths were in males.
Could it be put down to suicides? Well, I don’t think so. I am not arguing that the fact that the implementation of lockdown and quarantines impacted the nation’s mental health. During my placement in Children & Adolescence Mental Health Services in the summer of 2021, I was deeply saddened by the sheer number of attempted suicides I was seeing on the ward. Some children as young as 13 years old were on the ward for serious attempts on their life; an age where I was mostly preoccupied with video games.
I don’t think this rise in excess deaths is solely due to suicides due to the timing of the rise in deaths in young people. Studies have shown that suicides in young people happened after a month of the implementation of lockdown. We are instead seeing a rise in deaths in young men and teenagers since the beginning of May-June this year (using UK data), as indicated by the graph below. People aged 18 and over in England were being invited to book their first Covid-19 jab in June of this year, 16 and 17-year-olds were invited two months later in August.
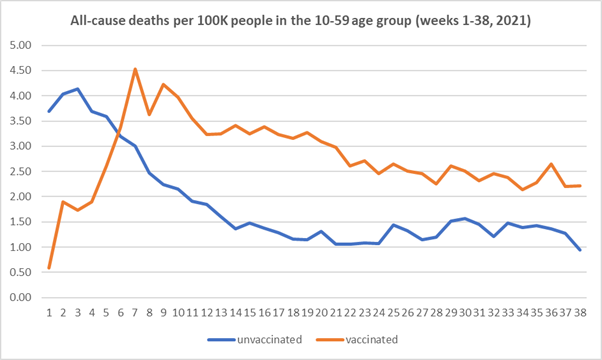
But as always, it’s hard to get a clear picture of what exactly is going on. The ONS are now publicly reporting age categorised all-cause death numbers by vaccination status. But, while it has data for age categories 60-69, 70-79 and 80+, there's only a single category of data for the age group 10-59. Not very helpful in my opinion.
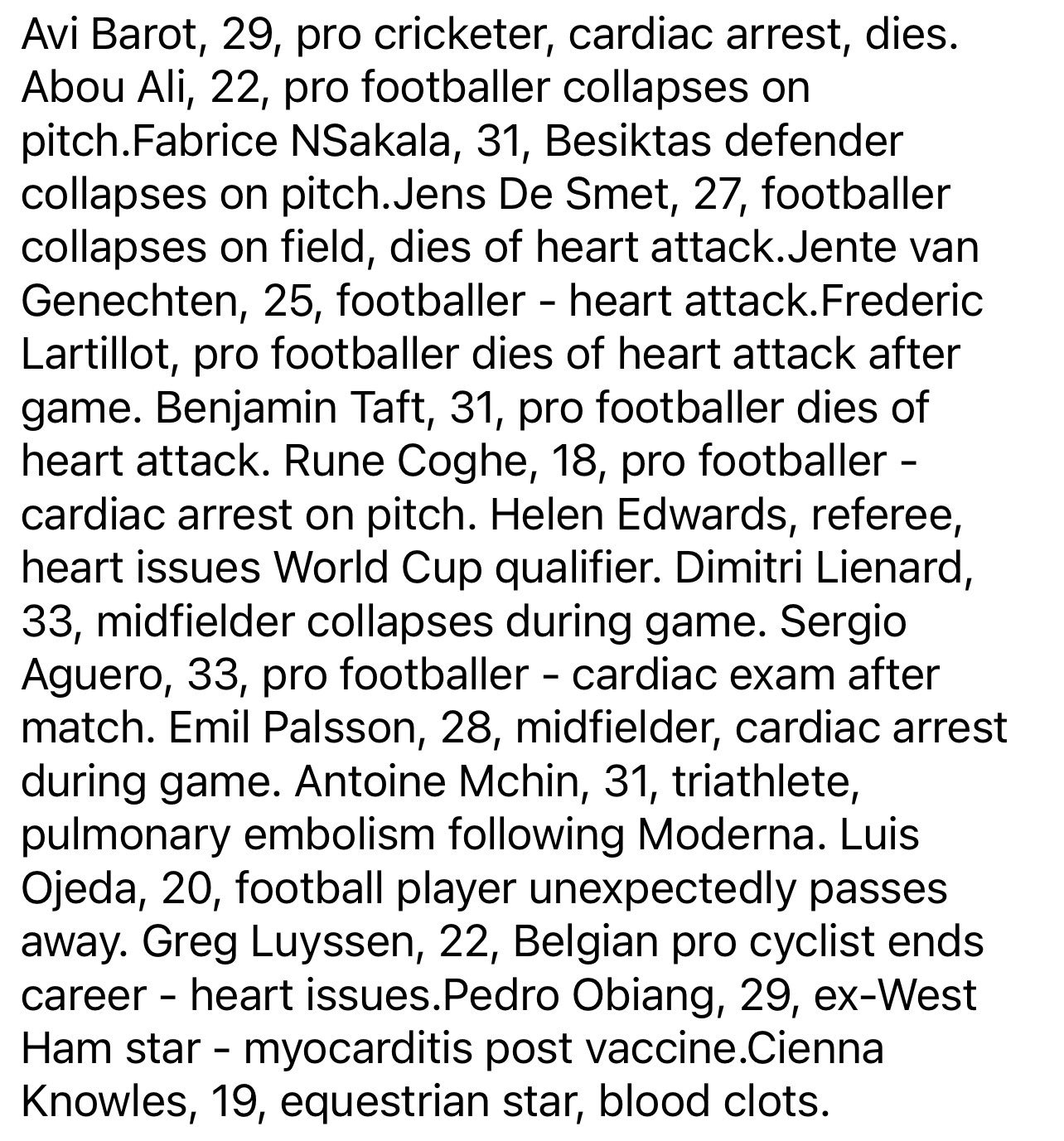
Raw data aside, we can’t ignore the increase in sudden deaths in young male athletes. One German news agency compiled a list of 75 European athletes who have died "suddenly" in the past 5 months since being fully vaccinated. To date (early November), there have been 54 collapses reported in sports games in the four and a half months since Christian Eriksen collapsed shortly before half-time in Denmark's opening Euro 2020 game against Finland. Of these 54 collapses, 30 resulted in death, almost all in 15-19-year-old players.
Though it is not uncommon for athletes to die from sudden death, usually secondary to cardiac hypertrophy, I worry that we are seeing more of these occur than we should. What could possibly be going on?
Myocarditis
We know that these vaccines are linked to myocarditis, an inflammation of the heart muscle. Myocarditis is a serious condition linked to fatal misfiring of the heart beat, heart failure and even sudden death. It seems like other countries have noted this risk and have halted the use of certain vaccines in young people. Not the UK or US however.
The worrying thing about myocarditis is that it can lay ‘dormant’, affecting people asymptomatically until it is too late. It is a condition with a mortality rate of 7-15% and accounts for up to 17% of sudden cardiac death in children younger than 16 years.
It seems like individuals who are vaccinated are more likely to develop myocarditis than those who haven't. One Isreali study showed that individuals vaccinated with Pfizer’s mRNA vaccine had a 3.24-times increased risk of myocarditis within 21 days of either the first or second dose compared to unvaccinated individuals. A US study showed that those aged 12-39 years old had a 9.8-times increased risk of myocarditis/pericarditis at days 1–21 of vaccination compared to those at days 22–42 of vaccination.
Due to the relatively short period of time in circulation as well as lack of postmortems, the underlying pathophysiological mechanisms of COVID vaccine-induced myocarditis is still unknown. Current theories of why some people suffer with myocarditis post-vaccination include:
Reinfection.
We mustn't forget that myocarditis is normally caused by viral infections, including SARS-CoV-2. We also know that individuals who’ve been vaccinated are still able to suffer with COVID again. Interestingly, vaccinating against SARS-CoV may actually enhance disease with reexposure. This is what was found in early animal studies for SARS-CoV-1 and Middle East respiratory syndrome coronavirus. Vaccinated animals had enhanced disease with reexposure to wild-type virus after vaccination likely due to non neutralizing antibodies resulting in enhancement of antibody-induced cellular cytotoxicity, also known as antibody-dependent enhancement of immunity.
This also brings up the importance of checking immunity status before getting injected, something that we did not do. Many of us would have unknowingly been naturally immune from the virus before vaccination, but many likely became unwell post-vaccine. In theory, that’s exposure to the spike/pathogen four times. Compounding damage cannot be ruled out.
Increased auto-antibodies and molecular mimicry.
A case report of a patient with myocarditis post-vaccination noted that the patient had higher levels of antibodies against some self-antigens. And it must be noted that historically, circulating heart-reactive autoantibodies have been reported at a higher frequency in patients with myocarditis. Autoantibodies are found more frequently in first-degree relatives of patients with cardiomyopathy than in the healthy population.
Another proposed mechanism for myocarditis is molecular mimicry between the spike protein of SARS-CoV-2 and self-antigens. The antibodies that the vaccinated produce against SARS-CoV-2 spike glycoproteins have been shown to cross-react with structurally similar human peptide protein sequences, including α-myosin. α-myosin is a type of cardiac muscle involved in active force generation. Mutations in α-myosin have been shown to be linked with congenital heart defects, dilated cardiomyopathy and hypertrophic cardiomyopathy.
Mode of injection.
A recent study examined the hearts, blood and other organ profiles of mice injected with Pfizer’s mRNA vaccine via the intramuscular (muscle) compared to the intravenous (vein) route. Mice that were given the vaccines intravenously suffered with ‘multifocal myopericarditis with elevated serum troponin, cardiomyocyte degeneration, and changes of both necrosis and apoptosis, adjacent inflammatory infiltrate of mononuclear cells, interstitial edema, and visceral pericardial calcification within two days post injection’. Basically, excessive cardiac damage. Concerningly the study also revealed ‘histopathological changes of myopericarditis deteriorated and became rather diffuse after the second dose boosting with either IV or IM administration 14 days after the first dose of priming.’. Repeated vaccinations may cause further cardiac damage.
Increased cardiac inflammation.
A recent study showed that the vaccines may directly damage heart muscles by dramatically increasing inflammation on the endothelium and T cell infiltration of cardiac muscle. The study concluded that this ‘may account for the observations of increased thrombosis, cardiomyopathy, and other vascular events following vaccination.’.
Why men?
There are many possible reasons why young men unfavourably develop vaccine-induced myocarditis compared to women. Firstly it is thought that oestrogen may have inhibitory effects on pro-inflammatory T-cells, resulting in a decrease in the body’s inflammatory immune responses. Pericarditis incidence is also higher in women during the postmenopausal period. One mouse study suggested that white adipose tissue (a type of body fat) may serve as a reservoir for SARS-CoV-2, sparing the lungs from the viral burden and infection severity. They note, ‘It is well documented that females have higher body fat content compared to males and the fat distribution pattern differs between the sexes, which constitute one reason why males are more susceptible to pulmonary CoV2 infection.’. More data is needed to confirm whether this is true with regard to cardiac damage.
Thinking out loud, I feel that younger fitter men (e.g. pro-soccer players) are more likely to suffer from post-vaccine myocarditis due to a combination of reasons. Young healthy men naturally tend to have lower body fat percentages, higher circulating testosterone levels, greater heart muscle mass and increased vascularity (increasing the risk of intravenous inoculation). Young men may also metabolise the mRNA vaccine ‘better’, creating more spike proteins than the average person. This may be why the Moderna vaccine is linked with a 2.5-times increased risk of myocarditis than Pfizer’s. Moderna’s mRNA vaccine dose (100 micrograms) is higher than Pfizer’s (30 micrograms).
My recommendation
What does this all mean then? Well, due to a lack of data, post-mortems to be specific, currently the link between vaccines and the increase in excess deaths in young people is still a correlation and not a causation. The correlation is strong however and we do know that these vaccines are linked to myocarditis and subsequent cardiac damage.
If you’re young and healthy, I’d ask you whether or not you are willing to risk your heart for a vaccine that you likely do not need. If unvaccinated, you’re likely naturally immune (even without you knowing) and let’s say that you aren’t already immune, then COVID-19 is very unlikely going to cause you serious harm. Remember too that vaccines do not prevent reinfection. Once you’re vaccinated, you cannot undo it. Life is precious and a damaged heart never makes full recovery. Whatever your decision may be, think long and hard about it first. Put your health first. But at the end of the day, it is your decision to make.